Links | About | Simon Moyes | Contact
- Surgeons site
- Treatment
- Historical Development
- Advantages and Contraindication
- Anatomy
- Instrumentation
- Theatre Layout
- Diagnostic Ankle Arthroscopy
Quick Search
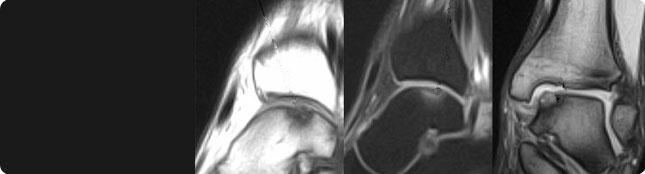
Osteochondral lesions of the talus - OLT
Osteochondral lesions of the talus as such were first described in 1856 Monro (36) but Konnig (37) coined the term ‘osteochondritis’ when he found similar pathology elsewhere in the body and thought the aetiology was osteonecrosis. Kappis (38) in 1922 first applied the term osteochondritis to the ankle joint.
Berndt and Harty (39) in 1959 postulated a traumatic aetiology and used the term transchondral fracture of the talus. O’Donoghue (40) said the lesions were intra-articular fractures and Campbell and Ranawat (41) felt the cause was ischaemia in 1966. Alexander and Lichtman (42) + Canale and Belding (43) have subsequently lent support to the traumatic aetiology in 1980. However the exact aetiology remains uncertain.
It is certainly a condition which tends to be under diagnosed bearing in mind that talar osteochondritis accounts for 4 -10% of all the osteochondritides. It affects males more commonly than females and a peak incidence at 20-30 yrs of age (44).
The lesions are either posteromedial or anterolateral. If they are posteromedial - 70% are traumatic - are deep and not usually displaced. They are usually caused by inversion of the dorsiflexed foot (torsional impaction) (45). Of the anterolateral lesions, 90% are traumatic - they are usually thinner and are more commonly displaced. They are typically caused by inversion of the plantar flexed foot (45).
Clinically, patients present with a history of trauma, pain, swelling, catching, giving-way or locking. On examination one may find swelling and tenderness.
The diagnosis is best made by CT or MRI according to Verhagen in 2005 (46). A classification based on CT correlates better with the arthroscopic findings than the original classification of Berndt and Harty (45, 47). Zinman (48, 49) and his colleagues found CT to be superior to XR’s in diagnosis, but MRI also has been advocated (50, 51) particularly by Dipaoala. Anderson has developed an MRI based classification and found CT to be as good as MRI except in diagnosing Grade 1 lesions (52).
Cheng and Ferkel (53) went on to show CT to be the scan of choice if the diagnosis is known but MRI if it is not. They have also developed an arthroscopic classification.
Treatment of the stages 1 & 2 lesions is 6-12 weeks in a cast, but arthroscopy if conservative treatment fails. Stages 3 & 4 lesions are treated arthroscopically immediately.
Results of treatment are good with Loomer (54) showing 80% good or excellent results. Of those patients who don’t do well, Takao M et al in 2004 (55) showed that debriding and re-drilling partially healed lesions produced improved outcomes in 93%.
The surgical approach is as follows for acute OLT. They are palpated with hook. Loose chondral fragments alone are excised but osteochondral fragments are pinned or screwed into the base of the defect whether displaced or undisplaced .
For chronic OLT, again palpate with a hook; see if it is loose. Fix it if it is loose and the underlying bone is healthy; if the underlying bone is unhealthy, you need to excise the loose fragment and drill the base of the defect. Large areas can be treated by osteochondral graft large.
It has been shown by Buckwalter that penetration of subchondral bone disrupts subchondral vessels (56-59), this produces bleeding , a clot and fibrocartilagenous repair (60, 51). The cells responsible for this enter from the marrow (62, 63). Significant cartilage defects can be repaired by tissue which grows up drill holes to cover exposed subchondral bone (64).
The results of arthroscopic treatment of OLT are as good if not better than open surgery (65-71) ie 80% plus.
Click here for a video of loose bodies
Click here for information on rehabilitation
References
(36) Monro A, ‘Microgeologie’ Berlin: Th Billroth, 1856:236
(37) Konnig F, ‘Veber freie Korper in den Gelenken’ Dtsch Z Chir 1888; 27:90
(38) Kappis M, ‘Weitere Beitrage zu traumatisch - mechanischen Enstehung der ‘spontanen’ Knorpelalblosungen sogen’ Dtsch Z Chir 1922; 171:13
(39) Berndt A L, Harty M, ‘Transchondral fractures of the talus’ JBJS 1959; 41A:988
(40) O’Donoghue D H, ‘Chondral and osteochondral fractures’ J Trauma 1966; 6:469
(41) Campbell C J, Ranawat C S, ‘Osteochondritis Dissecans : the question of aetiology’ J Trauma 1966; 6:201
(42) Alexander A H, Lichtman O M, ‘Surgical treatment of transchondral dome fractures. JBJS 1980; 62A:646
(43) Canale S T, Belding R H, ‘Osteochondral lesions of the talus’ JBJS 1980; 62A:97
(44) Thompson J P, Loomer R L, ‘Osteochondral lesions of the talus in a sports medicine clinic’ Am J Sports Med 1984; 12:460
(45) Berndt A L, Harty M, ‘Transchondral fractures of the talus’ JBJS 1959; 41A:988
(46) Ferkel R D, Sgaglione N A, ‘Arthroscopic treatment of osteochondral lesions of the talus: long term results’ Orth Trans 1993-1994; 17:1011
(47) Verhagen R A W, Maas M, Dijkgraaf M G W, Tol J L, Krips R, van Dijk C N, ‘Prospective study on diagnostic strategies in osteochodral lesions of the talus. Is MRI superior to helical CT?’ JBJS 2005; 87:1; 41-6
(48) Zinman C, Wolfson N, Reiss N D, ‘Osteochondritis of the dome of the talus’ JBJS 1988; 70A; 1017
(49) Zinman C, Reiss N D, ‘Osteochondritis of the talus : use of the high resolution computed tomography scanner’ Acta Orthop Scand 1982; 52:697
(50) Dipaoala J D, Nelson D W, Colville M R, ‘Characterising osteochondral lesions by magnetic resonance imaging’ Arthroscopy 1991; 7:101
(51) Nelson D W, Dipaoala J, Colville M R, Schmidgall J, ‘Osteochondritis dissecans of the talus and knee: prospective comparison of MR and arthroscopic classification’ J Comp Assist Tomography 1990; 14:804
(52) Anderson I F, Crichton K J, Grattan-Smith T et al, ‘Osteochondral fractures of the dome of the talus’ JBJS 1989; 71A:1143
(53) Cheng M S, Ferkel R D, Applegate GR ‘Osteochondral lesions of the talus : a radiologic and surgical comparison’ Presented at the AAOS Feb 1995
(54) Loomer R, Fischer C, Lloyd-Smith R et al, ‘Osteochondral lesions of the talus’ Am J Sports Med 1993; 21:13
(55) Takao M, Uchio Y, Kakimaru H, Kumahashi N, Ochi M, ‘Arthroscopic drilling with debridement of remaining cartilage for osteochondral lesions of the talar dome in unstable ankles’ Am J Sports Med 2004; 32:2; 332-6
(56) Buckwalter J A, Cruess R L, ‘Healing of the musculoskeletal tissues’ in (57) Rockwood C A Jr, Green D P, Bucholz R W eds, ‘Fractures in adults’ Philadelphia: J B Lipincott, 1991:181
(58) Buckwalter J A, Mow V C, ‘Cartilage repair in osteoarthritis’ In Moskowitz R W, Howell D S, Goldberg V M, Mankin H J eds, ‘Osteoarthritis: diagnosis and medical / surgical management’ Philadelphia; W B Saunders, 1992:71
(59) Buckwalter J A, Rosenberg L C, Hunziker E B ‘Articular cartilage: composition, structure, response to injury, and methods of facilitating repair’ In Ewing JW ed, ‘Articular cartilage and knee joint function: basic science and arthroscopy’ New York: Raven Press , 1990:19
(60) Johnson L L, ‘Arthroscopic abrasion arthroplasty , historical and pathological perspective: present status’ Arthroscopy 1986; 2:54
(61) Johnson L L, ‘The sclerotic lesion: pathology and the response to arthroscopic abrasion arthroplasty’ In Ewing J W, ed ‘Articular cartilage and knee joint function, basic science and arthroscopy’ New York: Raven Press, 1990:319
(62) Buckwalter J A, Cruess R L, ‘Healing of the musculoskeletal tissues’ In Rockwood CA Jr, Green D P, Bucholz R W eds ‘Fractures in adults’ Philadelphia: J B Lipincott, 1991:181.
(63) Shapiro E, Koide S Glimcher M J, ‘Cell origin and differentiation in the repair of full thickness defects of articular cartilage’ JBJS 1993; 75A:532.
(64) Mitchell N, Shepard N ‘The resurfacing of adult rabbit articular cartilage by multiple perforations through the subchondral bone’ JBJS 1976; 58A:230
(65) Mukherjee S K, Young A B, ‘Dome fractures of the talus - a report of ten cases’ JBJS 1973; 55B:319
(66) Naumetz V A, Schweigel J F, ‘Osteocartilagenous lesions of the talar dome’ J Trauma 1980; 20:924
(67) Pettine K A, Morrey B F, ‘Osteochondral fractures of the talus, a long term follow-up’ JBJS 1987; 69B:89
(68) Baker C L, Andrews J F, Ryan J B, ‘Arthroscopic treatment of transchondral talar dome fractures’ Arthroscopy 1986; 2:82
(69) Parisien J S, ‘Arthroscopic treatment of osteochondral lesions of the talus’ Am J Sports Med 1986; 14:211 .
(70) Van Buecken K P, Barrack M D, Alexander A H, Ertl J ‘Arthroscopic treatment of transchondral talar dome fractures’ Am J Sports Med 1989; 17:350
(71) Frank A, Cohen P, Beaufils P, Lamare J, ‘Arthroscopic treatment of osteochondral lesions of the talar dome’ Arthroscopy 1989; 5:57